Diagnostic imaging and other diagnostic tests play an important role in understanding the nature of neurological disorders. Advances in medicine, technology, and pharmacology have contributed to safer outcomes for children who may need sedation for diagnostic tests. Imaging or other tests may be performed to obtain a baseline for future studies.
In general, radiographic or digital imaging is looking at brain structure, while other diagnostic tests like electroencephalogram (EEG), single photon emission computed tomography scanning (SPECT),
nuclear medicine scans, and Wada tests are evaluating specific functions of the brain. Positron emission tomography (PET) scans look at metabolic function and utilization of glucose by the brain. Newer technologies allow for the evaluation of cerebral blood flow and brain perfusion. Some tests serve both diagnostic and therapeutic outcomes are:
X-rays of the skull and vertebral column; X-rays to look at boney structures of the skull and spine, fractures, integrity of the spinal column, presence of calcium intra-cranially. Patient should be immobilized in a collar for transport if there is a question of spinal fracture.
Cranial ultrasound; Doppler sound waves to image through soft tissue. In infants can only be used if fontanel is open. No sedation or intravenous access needed. Used to follow ventricle size/bleeding in neonates/infants.
Computerized tomography with/without contrast; Differentiates tissues by density relative to water with computer averaging and mathematical reconstruction of absorption coefficient measurements. Non-invasive unless contrast is used or sedation needed. Complications include reaction to contrast material or extravasation at injection site.
- Computerized tomography - bone windows and/or threedimensional reconstruction; Same as above with software capabilities to subtract intracranial contents to look specifically at bone and reconstruct the skull or vertebral column in a three-dimensional model. No changes in study for patient. Used for complex skull and vertebral anomalies to guide surgical decision-making.
- Cerebral angiography; Intra-arterial injection of contrast medium to visualize blood vessels; transfemoral approach most common; occasionally brachial or direct carotid is used. Done under deep sedation or anesthesia; local reaction or hematoma may occur; systemic reactions to contrast or dysrhythmias; transient ischemia or vasospasm; patient needs to lie flat after and CMS checks of extremity where injection was done are required.
MRI with or without contrast (gadolinium); Differentiates tissues by their response to radio frequency pulses in a magnetic field; used to visualize structures near bone, infarction, demyelination and cortical dysplasias. No radiation exposure; screened prior to study for indwelling metal, pacemakers, braces, electronic implants; sedation required for young children because of sounds and claustrophobia; contrast risks include allergic reaction and injection site extravasation.
MRA MRV; Same technology as above used to study flow in vessels; radiofrequency signals emitted by moving protons can be manipulated to create the image of vascular contrast. In some cases can replace the need for cerebral angiography; new technologies are making this less invasive study more useful in children with vascular abnormalities.
Functional MRI; Technique for imaging activity of the brain using rapid scanning to detect changes in oxygen consumption of the brain; changes can reflect increased activity in certain cells. Used in patients who are potential candidates for epilepsy surgery to determine areas of cortical abnormality and their relationship to important cortex responsible for motor and speech functions.
SPECT; Nuclear medicine study utilizing injection of isotopes and imaging of brain to determine if there is increased activity in an area of abnormality; three-dimensional measurements of regional blood flow. Often used in epilepsy patients to diagnoses areas of cerebral uptake during a seizure (ictal SPECT) or between seizures (intraictal SPECT).
SISCOM; Utilizing the technology of SPECT with MRI to look at areas of increased uptake in conjunction with MRI images of the cortex and cortical surface. No significant difference for patient; software as well as expertise of radiologist is used to evaluate study.
PET; Nuclear medicine study that assesses perfusion and level of metabolic activity of both glucose and oxygen in the brain; radiopharmaceuticals are injected for the study. Patient should avoid chemicals that depress or stimulate the CNS and alter glucose metabolism (e.g., caffeine); patient may be asked to perform certain tasks during study.
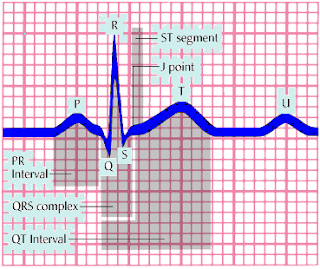
- EEG Routine Ambulatory Video; Records gross electrical activity across surface of brain; ambulatory EEG used may be used for 24–48 h with data downloaded after study; video combines EEG recording with simultaneous videotaping. Success of study dependent on placement and stability of electrodes and ability to keep them on in children; routine studies often miss actual seizures but background activity can be useful information.
Evoked responses;SSER;VER;BAER ; Measure electrical activity in specific sensorypathways in response to external stimuli; signal average produces waveforms that have anatomic correlates according to the latency of wave peaks. Results can vary depending on body size, age and characteristics of stimuli; sensation for each test will be different for patient – auditory clicks (BAER), strobe light (VER), or electrical current on skin – somatosensory (SSER).
Read More